Provision of a maxillary cobalt chromium based partial denture/protective occlusal splint in a heavily restored dentition
Diagnoses:
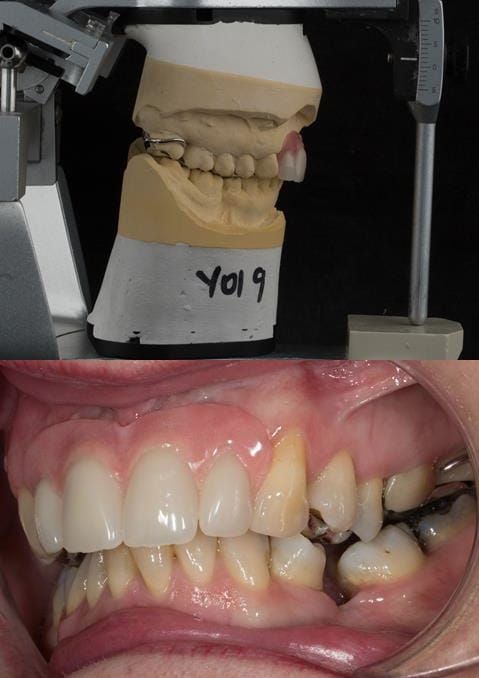
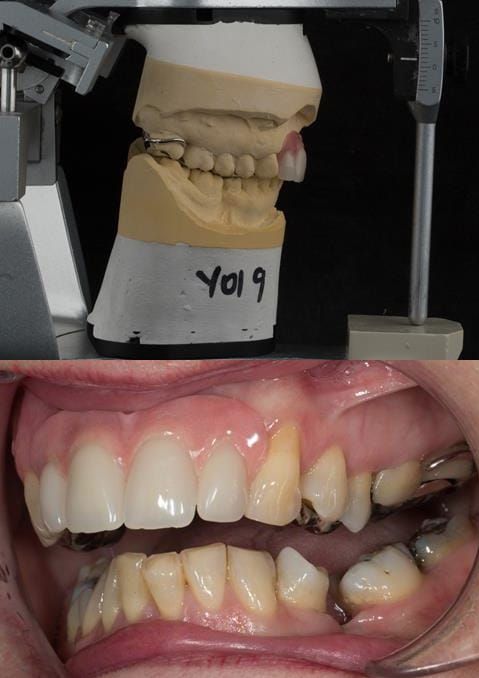
- UR2 peri-radicular periodontitis with a peri-radicular area on the root apex. Retrograde amalgam filling from a previous apicectomy. No visible root canal or root canal filling. Large circumferential marginal gap between the crown and tooth. Large post and core present. Very little tooth structure remaining resulting in a fragile tooth with increased potential for fracture.
- UR1 peri-radicular periodontitis with a small peri-radicular area on the root apex with wide blunderbuss apex. Radio-opaque root canal filling present approximately 3 mm short of the radiographic apex. Large circumferential marginal gap between the crown and tooth. Large post and core present. Very little tooth structure remaining resulting in a fragile tooth with increased potential for fracture.
- UL1 peri-radicular periodontitis with a peri-radicular area on the root apex. Retrograde amalgam filling from a previous apicectomy. Visible root canal space with no sign of root canal filling. Large circumferential marginal gap between the crown and tooth. Large post and core present. Very little tooth structure remaining resulting in a fragile tooth with increased potential for fracture.
- UL2 peri-radicular periodontitis with a peri-radicular area on the root apex. No visible root canal or root canal filling. Large circumferential marginal gap between the crown and tooth. Large post and core present. Very little tooth structure remaining resulting in a fragile tooth with increased potential for fracture.
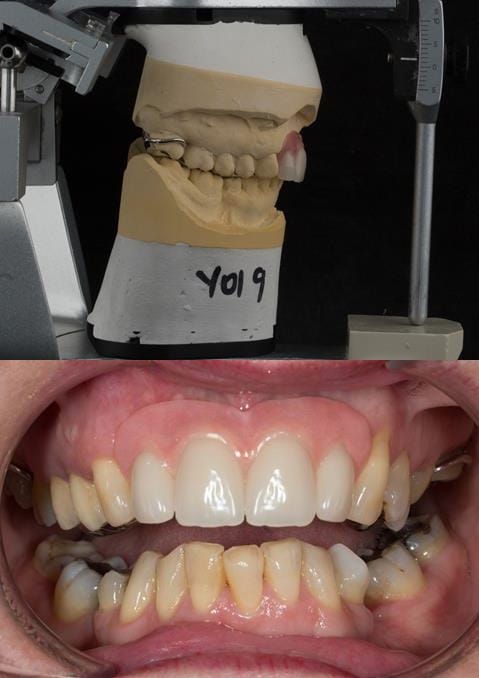
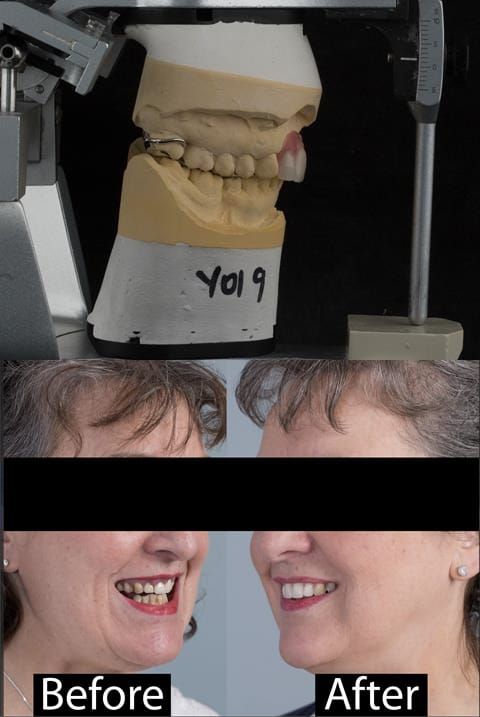
- High smile line showing gum above gingival zeniths of upper front teeth when smiling. Aesthetic failure of the upper four incisors with inflammation of the gingivae and mis-match of the gingival zenith levels.
- Other than the maxillary incisors the remaining dentition was in marginally better condition being moderately to heavily restored. Many will probably require replacement and restoration from time to time mainly from wear and tear owing to occlusal forces.
Treatment options discussed with the patient:
- Do nothing. The patient did not want this option.
- Strip down the upper anterior teeth to investigate their restorability, root canal treat as necessary, place new post and cores, fit well adapted provisional crowns, muco-gingival surgery to level the gingival margin zeniths and place definitive crowns. One or more of these teeth may not be restorable - if so replace with a dental implant supported crown (s). The patient did not want to have this option as she did not want to risk future failure of the restored teeth.
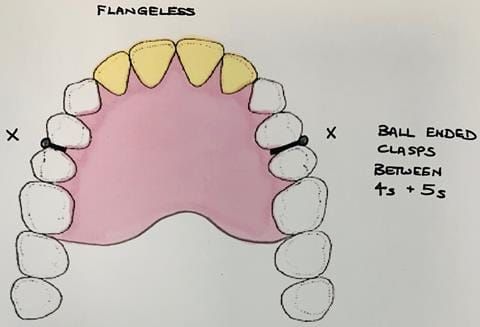
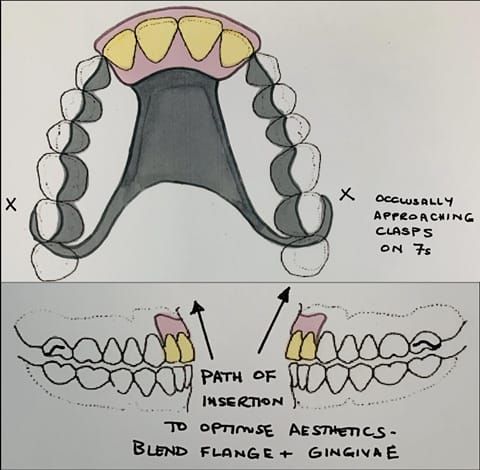
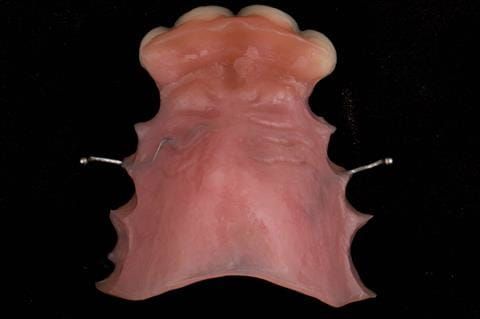
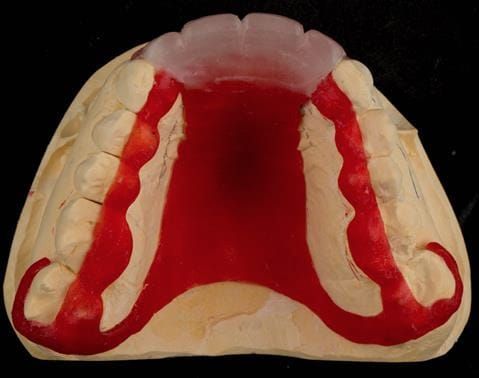
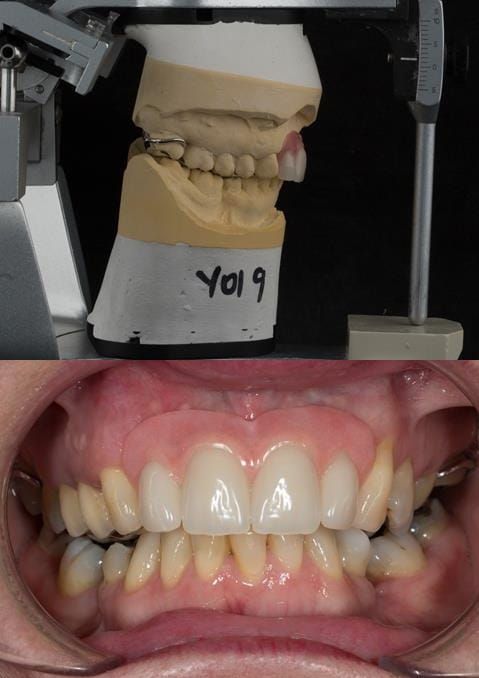
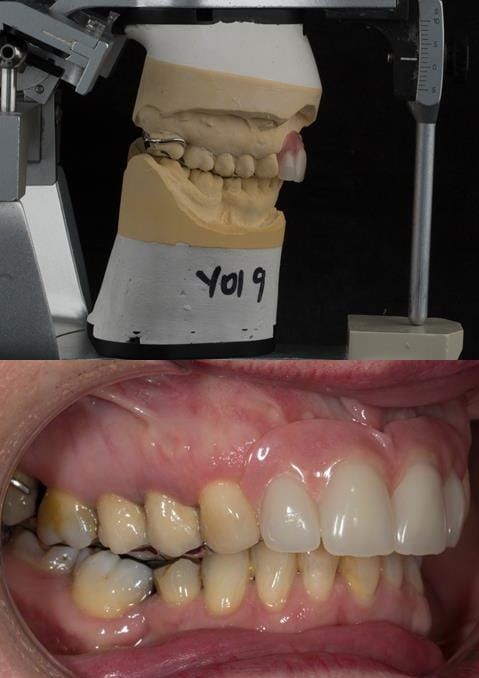
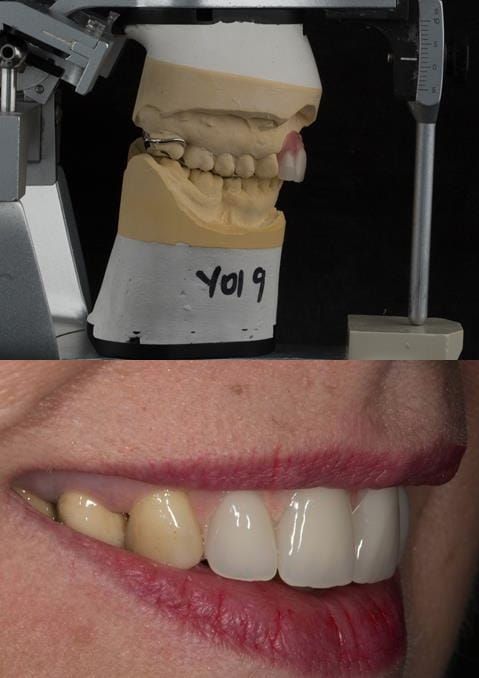
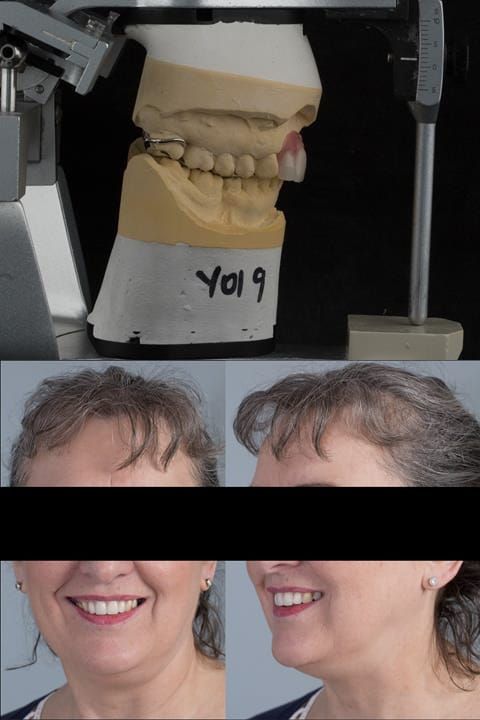
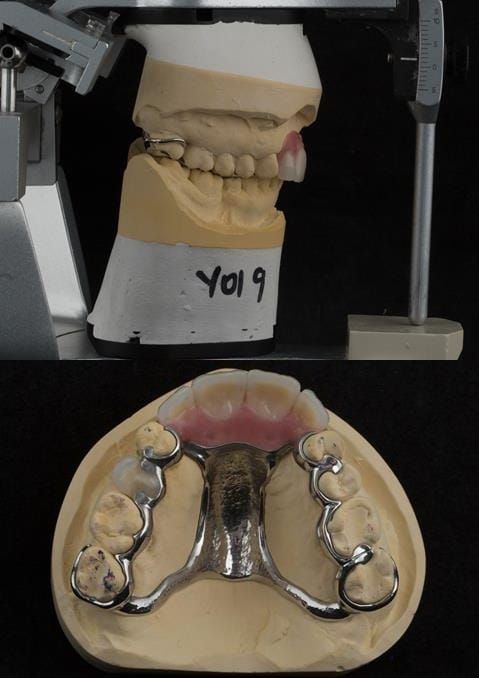
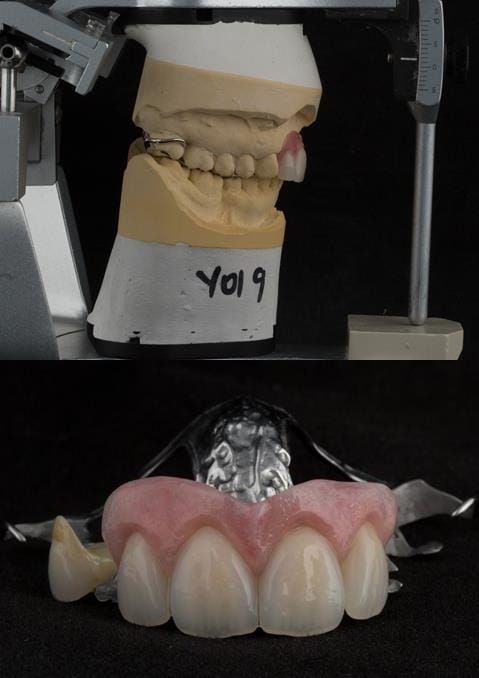
- Extract the upper 2-2 teeth and replace with an interim acrylic based partial denture. Reline the interim denture over 9 - 12 months, replacing with a definitive cobalt chromium based partial denture. The definitive denture would ideally be designed as an occlusal protective splint to reduce the the potential for mechanical wear and breakages of the moderately/heavily restored maxillary dentition. In addition, should further upper teeth require extraction they could be added on to the denture cobalt chromium framework - therefore a new prosthesis would not be required as future teeth are lost. This option would produce an excellent aesthetic outcome. This is the option the patient chose to have.
- Extract the upper 2-2 teeth and replace with dental implant supported restorations in the form of bridge or individual crowns. The patient did not wish to have this option owing to financial constraints.
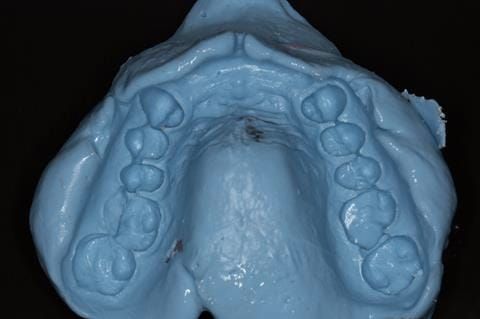
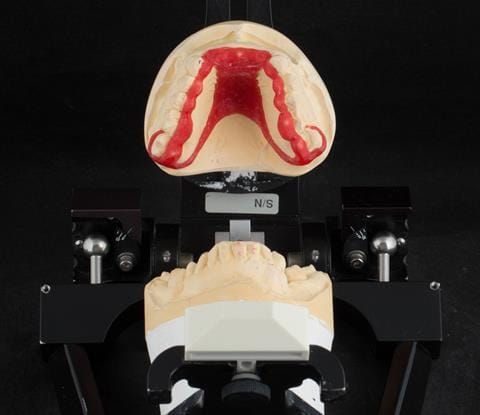
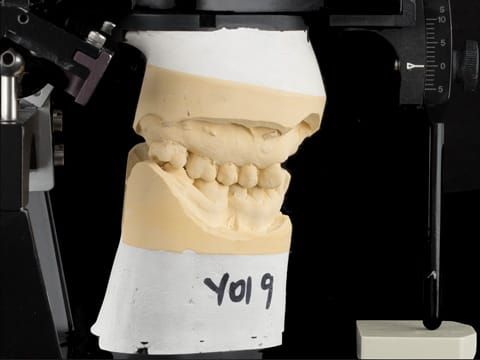
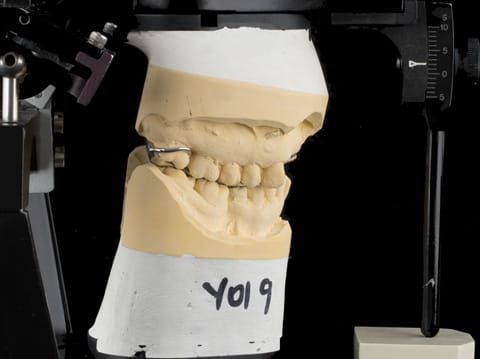
Following consultation and second discussion appointment the patient chose to have option 3 namely, a maxillary cobalt chromium based partial denture/protective occlusal splint. The clinical situation and treatment process is shown in detail below with photographs. The patient was successfully rehabilitated with this and her quality of life considerably improved. The clinical work was provided by Finlay and the technical work by Rowan.